Microlaryngoscopy
A microlaryngoscopy is an operation where the larynx (voicebox) is examined with magnification using a microscope or endoscope. This is carried out through the mouth using specialised instruments and if appropriate surgery is undertaken on the voice box.
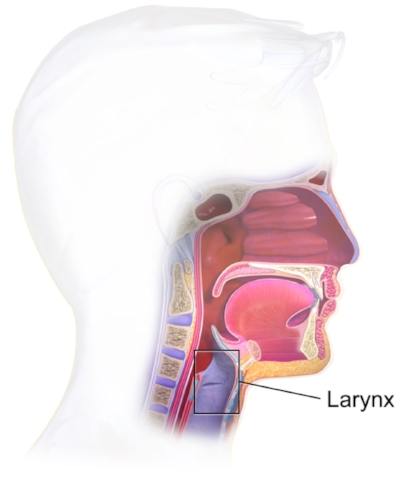
What is the larynx?
The larynx or voicebox is the area at the top of our trachea (windpipe) that contains the vocal cords. These are responsible for helping us speak. You can think of the lungs as the bellows that drives air to the larynx, the vocal cords as the tone generator that makes a sound, our mouth, lips and tongue as the modifiers articulate this sound to create speech and finally our nose and sinuses as hollows that give resonance to our speech. Consider how your voice sounds when you are experiencing a blocked nose.

More importantly, our larynx acts as a specialised protective system that prevents food passing through the trachea and into our lungs when we swallow. When this protective mechanism fails (aspiration) such as following a stroke, people may experience recurrent chest infections.
What are the reasons that a microlaryngoscopy may be undertaken?
To examine the vocal cords in detail
To assess the extent of growths involving the larynx
To remove cysts, swellings or tumours involving the vocal cords
To inject the vocal cords to help with voice weakness due to a paralysed vocal cord
What happens before the operation?
In your consultation with Dr. Michael, he will ask questions in relation to issues that you may be having with your voice. You will also have an endoscopy. This is a specialised examination where a fine camera (endoscope) is passed through the nose and then looks down into the larynx. Other tests such as specialised scans may also be arranged. Dependent upon what is found, Dr. Michael may consider conservative management options before advising upon surgery.
What does a microlaryngoscopy operation involve?
A microlaryngoscopy operation is undertaken with general anaesthesia and performed through the mouth without any external cuts.
Specialised intruments are passed through the mouth and then the vocal cords are examined either with an operating microscope or an endoscope. Fine instruments are then used to operate upon the vocal cords if indicated.
Are there any risks to having a microlaryngoscopy?
There are general risks associated with having an operation. These include nausea and vomiting, bleeding, infection and allergies to medicines or dressings used. When having an operation under general anaesthesia, other risks include blood clots in the legs or lungs, a stroke or a heart attack. However, the risk of these serious complications is extremely low. Your anaesthetist will discuss these with you prior to the operation.
With regards to microlaryngoscopy, there are a number of specific risks. These are listed below.
The operation is undertaken through the mouth using metal surgical instruments. Consequently, there is a potential risk of damage to surrounding structures such as the lips, gums, teeth and tongue. This risk is extremely small and shields are used to protect the teeth. However, the risk increases in those who have loose teeth or when there are large gaps between teeth due to missing teeth.
Some lesions in the larynx can be removed but have a potential to recur. This risk will vary depending upon the lesion that you have and Dr Michael will discuss these risks with you during your consultation. In particular, continued smoking has increases the risk of recurrence of a number of lesions and therefore the importance of smoking cessation cannot be stressed enough.
The aim of some operations on the larynx is to improve an individual’s voice. However, on occasion, the voice can be worse. This can occur due to scarring occurring in the vocal cord. During the operation, techniques will be employed to reduce this risk. Further, if there are lesions affected both vocal cords, you will most likely be recommended to have two operations over a period of time to allow one vocal cord to heal before the other is operated upon. This is again to reduce of scar formation occurring between the vocal cords. We term this an acquired laryngeal web.
Occasionally this issues may mean that a revision operation may be required.
Very rarely, if there are issues with airway obstruction at the level of the larynx, a tracheostomy may be required. This is an operation where an opening is made directly into the trachea (windpipe) in the lower part of the neck to bypass the airway obstruction and allow airflow to the lungs.
What happens after the operation?
There is usually minimal discomfort and you may require an overnight stay dependent upon the issue with the larynx, your general health and social circumstances.
You will be seen at regular intervals to assess for complications and assess your progress.
Are there any precautions that I should undertake?
It is vital that you stop smoking at least 2 weeks before the operation. Following your operation, you will be instructed upon a period of voice rest. This will no talking or whispering for the first 48 hours, speaking in a quiet voice (without whispering) for 1 week and then gradually returning in volume to your normal voice. During this time, you should drink water regularly, not return to smoking and cough or undertake strenuous activity.